"Tell me about a patient you remember rooming who was clearly anxious or upset before the provider came in. What did you actually do?"
VeraHire Hiring GuidesMedical AssistantUpdated 2026
How to hire a Medical Assistant in 2026
TL;DR
Great medical assistants are made of clinical accuracy, calm bedside manner, and judgment about what they can and can't do — not resume keywords. The fastest way to find them is to stop asking hypotheticals and start asking for real past behavior at the chairside and front desk, then score every answer against the same criteria. Below are the 8 interview questions that actually predict MA performance, what to listen for, the red flags, and how VeraHire scores each one automatically.
The role, honestly
What a great Medical Assistant actually does
The job title hides how varied the work is. A strong MA is part clinician's hands, part patient advocate, part front-office operator — switching between all three many times an hour.
On paper a medical assistant "supports the care team." In practice the role splits into two halves that rarely sit still: clinical work — taking vital signs, drawing blood, giving injections, rooming patients, prepping instruments — and administrative work — scheduling, verifying insurance, updating the EHR, and managing the phones. In a small primary-care practice one MA may do all of it before lunch; in a larger specialty group the clinical and administrative tracks are often split between people. Knowing which version of the job you're hiring for changes everything about who you screen for.
The best ones make a chaotic clinic feel orderly. They get an accurate blood pressure on the first try, document exactly what the provider needs, and notice when a "routine" patient is actually short of breath. They put a nervous patient at ease before a needle, follow infection-control protocol even when the schedule is slipping, and never guess at something outside their scope — they ask.
Clinical tasks done right
Take accurate vitals, perform venipuncture and capillary draws, administer injections and give vaccines per protocol, run EKGs, and prep specimens — within their state scope and the provider's order.
Patient intake & rooming
Greet, room, and prepare patients; collect history, medications, and chief complaint accurately; and set the tone so anxious patients arrive at the provider already calmer.
EHR & administrative flow
Document encounters cleanly in the EHR, handle scheduling and insurance verification, route messages and refills, and keep the day moving without dropping charts or callbacks.
Infection control & empathy
Follow hand hygiene, PPE, and sterilization protocol every time, manage exam-room turnover safely, and read the room — meeting fear, pain, or confusion with steady reassurance.
The unique data
The interview questions that actually predict performance
Eight medical-assistant-specific questions built around past behavior, not hypotheticals. For each one: what to listen for, the red flag that should worry you, and a follow-up probe to pressure-test the answer.
"Describe a time a patient refused a blood draw or injection, or panicked partway through. Walk me through exactly what you said and did."
"On a fully booked day with patients backing up, how do you make sure a vital sign or a medication entry doesn't get recorded wrong?"
"You're taking vitals and something looks off — a very high blood pressure, or a patient who suddenly seems unwell. What happens next?"
"Walk me through how you turn over an exam room between patients, and a time you saw a contamination or sterility risk and what you did."
"A patient asks you what their lab results mean, or to adjust their medication dose. What do you do?"
"Tell me about the EHR you used most and how you kept documentation accurate when the clinic was slammed."
"Clinics are long days of back-to-back patients, some of them in pain or upset. How do you stay accurate and kind by the last appointment?"
Evidence-based scoring
How VeraHire scores each answer
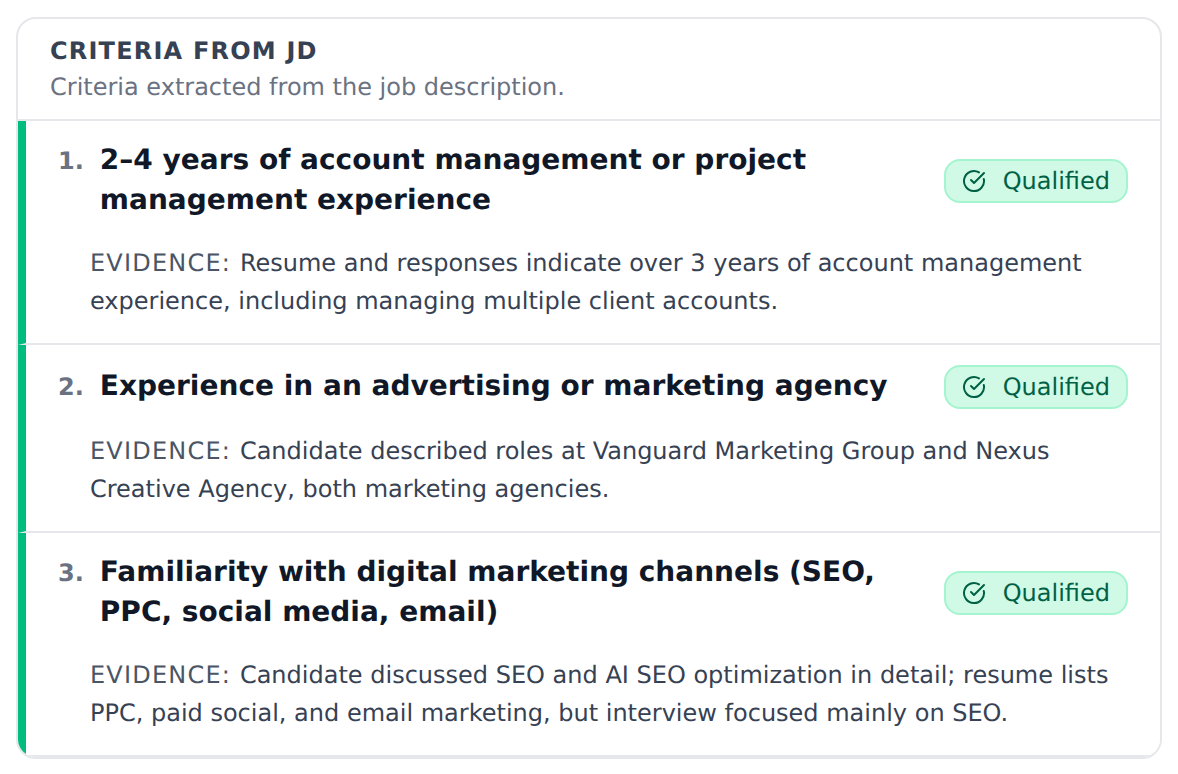
Good questions are only half the job. VeraHire turns the job description into explicit criteria, then scores every candidate's answer against them — with the evidence cited, so the score is auditable instead of a gut feeling.
When you run a medical assistant interview, VeraHire extracts the must-have criteria from your job description — clinical accuracy, scope-of-practice judgment, infection-control discipline, bedside manner, EHR fluency — and marks each one Qualified or Not Qualified based on what the candidate actually said. Every verdict links back to the exact moment in the transcript that supports it, so a clinic manager or lead provider can verify the call in seconds rather than re-listening to a recording.
Compensation snapshot
What does a Medical Assistant typically cost?
Pay varies widely by region, setting, certification, and experience. Use the range below to sanity-check your budget — then confirm against an authoritative source before you post.
$44,200
median US wage / year (BLS, 2024)
The US median wage for medical assistants is $44,200 per year (about $21.25 per hour) as of May 2024. Most fall between roughly $35,020 and $57,830 (10th–90th percentile) — entry-level and rural roles toward the lower end, and certified, experienced, or specialty-clinic MAs in higher-cost metros toward the upper end.
Treat these as planning figures — actual market rates shift by city, specialty, and year, and certification (CMA, RMA, CCMA) and outpatient versus hospital settings change the math.
Source: U.S. Bureau of Labor Statistics, OEWS — May 2024
Avoid these
Common mistakes when hiring medical assistants
Most bad MA hires trace back to the same handful of screening shortcuts.
- i.Ignoring certification and credential status. CMA, RMA, and CCMA aren't interchangeable, and some states and payers require specific credentials for certain tasks. Confirm the actual certification and that it's current — not just "certified" on a resume.
- ii.Treating an externship like real experience. A 160-hour program externship is valuable, but it isn't the same as running a live panel of patients. Probe what they did unsupervised versus observed.
- iii.Not separating clinical from administrative fit. Someone great at the front desk may be shaky with a needle, and vice versa. Hire against the actual mix of duties in your clinic, not a generic "MA."
- iv.Never testing scope-of-practice judgment. An MA who improvises medical advice to be "helpful" is a liability. If no question probes where they stop and defer, you learn nothing about their judgment.
- v.Asking only hypotheticals. "What would you do if a patient panicked?" rewards good talkers. "Tell me about a patient who panicked" reveals real chairside behavior.
- vi.Skipping bedside manner entirely. Clinical skill with no warmth drives patients away. If nothing in your process reveals how they treat a scared patient, you're guessing on half the job.
Try it on your role
Generate a free first-round interview for your Medical Assistant role
Paste your job description, get a structured medical assistant interview with built-in scoring criteria, and start ranking real candidates in minutes — no ATS required.
FAQ
Hiring a medical assistant: quick answers
Does a medical assistant need to be certified?
It depends on your state and the tasks involved. Many states don't legally require certification to work as an MA, but a growing number — and most employers and payers — prefer or require a recognized credential such as the CMA (AAMA), RMA (AMT), or CCMA (NHA), and certain duties like giving injections may hinge on it. Confirm your state's rules and your payers' requirements, then verify the candidate's certification is current rather than trusting the resume.
Should I hire for clinical or administrative skills?
Decide which version of the job you're filling before you screen. Clinical MAs take vitals, draw blood, give injections, and room patients; administrative MAs handle scheduling, insurance, EHR, and the front desk. Many small practices need a blend, but the strongest candidate for one side isn't automatically strong on the other — interview against the actual mix of duties in your clinic.
What interview questions actually reveal a great medical assistant?
Past-behavior questions beat hypotheticals. Ask for a specific time they calmed a scared patient, handled a refused blood draw, caught a vitals or charting error, escalated an abnormal finding, or deferred a question that was outside their scope. Listen for accuracy, infection-control discipline, scope awareness, and genuine warmth — and probe with a follow-up on each.
How long does it take to hire a medical assistant?
It often runs about three to five weeks from posting to a started hire, factoring in credential and reference checks and any required background or immunization clearances. The slowest step is usually first-round screening — running structured, automatically scored interviews up front compresses that significantly so you spend live time only on qualified candidates.